How to Recover From Mental Burnout: A Psychologist’s Guide

Back in the day, I’d lecture my students on the dangers of chronic workplace stress: high workloads, low control, poor coping mechanisms. I remember drawing neat diagrams of the stress response on whiteboards, explaining the Social Readjustment Rating Scale, demonstrating biofeedback techniques. What was causing the peculiar cognitive collapse that accompanies chronic stress? Not just tiredness or reduced motivation, but genuine impairment: your working memory fails, concentration becomes impossible, executive function simply… stops.
The cause? Mental burnout. And knowing how to recover from mental burnout properly — not just push through it — makes the difference between weeks of recovery and months.
Burnout isn’t just feeling tired or stressed. It’s a state of cognitive impairment caused by chronic workplace stress that hasn’t been successfully managed. Research shows measurable deficits in memory, attention, executive function, and processing speed. Your brain literally stops functioning at its normal capacity.
The good news? These changes are reversible. Brain imaging studies show that with proper recovery, the structural and functional changes caused by burnout can be repaired. But recovery requires more than just a holiday. It requires systematic restoration of depleted cognitive resources. This guide provides evidence-based strategies for genuine recovery — not just symptom management.
How to Recover From Mental Burnout: Understanding What’s Happening to Your Brain
The World Health Organization defines occupational burnout as a work-related phenomenon resulting from chronic workplace stress that hasn’t been successfully managed. It’s characterised by three core dimensions: feelings of energy depletion or exhaustion, increased mental distance from your job (cynicism), and reduced professional efficacy.
Critically, burnout isn’t recognised as a medical condition — it’s classified as an “occupational phenomenon.” However, several European countries do recognise it clinically, and there’s substantial evidence that what we call burnout overlaps significantly with depressive conditions.
Swedish researchers investigating a surge of depression-related insurance claims found that many cases didn’t match typical depression presentation. Fatigue and decreased cognitive ability dominated, with people believing their working conditions were the cause. This led to identification of what’s now called clinical burnout or exhaustion syndrome.
The cognitive impacts are substantial and measurable. Meta-analysis shows burnout is associated with impaired episodic memory, short-term and working memory, executive function, attention and processing speed, and fluency. You’re not imagining it when work feels harder. Your cognitive machinery genuinely isn’t working properly.
The Six Drivers of Mental Burnout: Maslach’s Model
Psychologist Christina Maslach, whose work essentially created the field of burnout research, identified six workplace factors that contribute to burnout: workload, control, reward, community, fairness, and values. Burnout emerges when one or more of these is chronically mismatched between you and your job. It’s not just about working too much. As physician Richard Gunderman described it, burnout is “the accumulation of hundreds or thousands of tiny disappointments, each one hardly noticeable on its own.”
Understanding which factors are driving your burnout is essential for recovery. You can’t fix the problem without diagnosing which environmental mismatches are depleting your resources.
- Workload — too much to do in too little time. But it’s rarely just quantity. It’s also about the cognitive demand of the work relative to available resources.
- Lack of Control — autonomy over how you do your work. Lack of control is particularly toxic because it creates learned helplessness — you stop believing your actions matter.
- Absence of Reward — not just salary, but recognition, appreciation, and a sense that your work is valued. When effort consistently goes unacknowledged, motivation depletes.
- Lack of Community — relationships with colleagues. Isolation, conflict, or lack of support accelerates burnout. See my article on social connection and brain health.
- Unfairness — perceived justice in resource allocation, decision-making, and treatment. Chronic unfairness creates moral injury that’s exhausting to navigate.
- Values — misalignment between your values and organisational actions. When there’s a mismatch, you experience constant cognitive dissonance.
Why You Can’t Just “Power Through” Mental Burnout
Trying to recover from mental burnout by simply working harder and sleeping less is catastrophically counterproductive.
Every person’s mental and physical energy resources are finite. Mental energy is your inner psychological capacity for cognitive and emotional work. When demands chronically exceed your capacity to recover, resources deplete progressively.

Crucially, burnout isn’t a linear process. Research by Dutch psychologist Wilmar van Dam shows it progresses through qualitatively different phases: lack of recovery, changes in stress physiology, chronic stress symptoms, pseudo-psychopathology, and finally clinical burnout. In early phases, you can still function — you’re just running on depleted reserves. But if you continue without recovery, you cross a threshold into clinical burnout where cognitive function measurably impairs. At this stage, “just trying harder” makes things worse.
Brain imaging reveals why. Long-term occupational stress is associated with reduced brain tissue volume in the prefrontal cortex, amygdala, and other regions. These aren’t temporary, reversible changes from today’s workload — they’re structural adaptations to chronic stress. The good news? A study of medical students during intensive exam preparation showed that after four weeks of recovery, brain changes normalised. Recovery at the neurological level is possible. But it requires actual recovery, not just wishful thinking.
QUICK WIN:
If you’re currently burnt out, identify which of Maslach’s six factors — workload, control, reward, community, fairness, or values — is the biggest mismatch in your current role. Write it down. This single act of naming the cause begins to separate the problem from your identity, which is the first step toward addressing it.
Phase 1: Immediate Stabilisation — The First Step to Recovering From Mental Burnout (Weeks 1–2)
If you’re in clinical burnout, recovery begins with stabilisation. You cannot restore function whilst continuing to deplete resources. This phase requires difficult decisions.
Reduce cognitive load immediately. This might mean taking sick leave, reducing hours, or delegating responsibilities. I know this feels impossible — that’s the burnout talking. When your brain can’t function properly, continuing to make high-stakes decisions from a depleted state creates more problems than it solves. Research shows alternating complex cognitive tasks with simpler ones reduces mental fatigue. If you absolutely cannot reduce overall workload, at least restructure your day. Schedule demanding cognitive work during your peak hours. Batch similar tasks. Build in recovery breaks between high-demand activities.
Protect sleep as sacred. Sleep disruption is both a symptom and a perpetuating factor in burnout. Poor sleep impairs cognitive function significantly, creating a vicious cycle. See my guide on sleep and cognitive function for evidence-based strategies. During stabilisation, aim for eight to nine hours nightly — more than usual. Your brain is repairing damage. This isn’t indulgence; it’s neurological rehabilitation.
Implement micro-recovery breaks. Research on workplace cognitive recovery shows that micro-breaks — short periods of genuine rest — help restore mental resources. These aren’t additional cognitive activities like reading or “productive” tasks. They’re actual rest: short naps, walking, stretching, listening to music, daydreaming. Schedule five to ten minute breaks every 90 minutes. Put them in your calendar. Treat them as seriously as meetings.
Nutrition and hydration basics. Burnout often coincides with degraded self-care. Your brain uses 20% of your body’s energy despite being 2% of body weight. When you’re running on coffee and skipping meals, you’re literally starving your brain of fuel. For detailed guidance, see my article on hydration and brain function.
Phase 2: Cognitive Rehabilitation — Rebuilding After Mental Burnout (Weeks 3–8)
Once you’ve stabilised — stopped actively getting worse — you can begin rebuilding cognitive capacity. This phase typically takes four to six weeks but varies substantially by severity.
Structured cognitive recovery through exercise. Physical exercise provides one of the most robust interventions for burnout recovery. Research shows significant cognitive improvements following exercise programmes, particularly for executive function and memory. Start gently if you’re depleted — even 20–30 minutes of walking shows benefits. The goal isn’t fitness; it’s neurological repair through increased BDNF (brain-derived neurotrophic factor) and improved cerebral blood flow. See my guide on exercise and brain health for protocols. Consistency trumps intensity during recovery. Daily gentle movement (such as walking your dog in the park) beats sporadic intense sessions.

Cognitive behavioural approaches. CBT specifically adapted for burnout shows effectiveness, though research quality is still developing. The core principle is restructuring maladaptive thinking patterns that perpetuate burnout. Common cognitive distortions in burnout include catastrophising (“If I don’t finish this, everything will collapse”), personalisation (“This is all my fault”), and all-or-nothing thinking (“If I’m not performing perfectly, I’m failing”). Working with a psychologist who understands occupational burnout can help identify and modify these patterns. However, cognitive restructuring alone isn’t sufficient if your workplace conditions remain toxic.
Mindfulness and stress management. Mindfulness-based interventions show moderate effectiveness in reducing burnout symptoms. The mechanism appears to be positive reappraisal of work stressors — mentally assigning them more benign interpretations — which enhances resilience and restores sense of meaning. For practical techniques, see my guides on mindfulness for focus and stress management for mental performance. Start with ten minutes daily. Consistency matters more than duration.
Rebuilding working memory and executive function. Targeted cognitive training can help restore impaired functions. Focus on practical, real-world tasks rather than abstract brain training games. Strategies that help include external memory aids (written task lists, calendar systems), breaking complex tasks into smaller steps, working memory strategies, single-tasking rather than multitasking, and reducing environmental distractions. For workspace optimisation, see my article on creating environments that support cognitive function.
QUICK WIN:
Schedule one 20-minute walk outdoors today — not as exercise, but as prescribed neurological recovery. Leave your phone in your pocket. Notice your surroundings. This is the single most accessible cognitive rehabilitation tool available to you, and it costs nothing.
Phase 3: Environmental Modification — Preventing Mental Burnout From Recurring (Ongoing)
Individual recovery strategies are necessary but not sufficient. If you return to the same conditions that caused burnout, you’ll deplete again. Environmental change is essential.
Workplace modifications. Research shows that burnout interventions exclusively using CBT reduce psychological symptoms but don’t effectively support return-to-work. Adding work-related exercises — reintegration planning, problem analysis of work situations — significantly improves outcomes. Practical modifications might include renegotiating workload, setting clearer boundaries, adjusting working hours, requesting role changes, or improving team communication. The goal is addressing the mismatches in Maslach’s six factors.
This requires difficult conversations. If you’re conflict-averse — and many burnout sufferers are — consider whether avoiding these conversations is worth continued cognitive impairment. For guidance on navigating workplace boundaries, see my article on saying no at work without burning bridges.
When to leave. Sometimes the environment is fundamentally incompatible with your wellbeing — toxic cultures, unrealistic demands, or values misalignment that senior leadership won’t address. Leaving feels like failure, especially when you’re burnt out and your executive function is impaired. But staying in an environment that chronically depletes you is choosing continued brain damage over short-term discomfort. If you’re contemplating leaving, ensure you’ve genuinely recovered first. Making major career decisions from a depleted state often leads to regrettable choices. Stabilise, recover cognitive function, then decide.
Building resilience systems. Once recovered, focus on systems that prevent recurrence. These include regular monitoring of energy levels, non-negotiable recovery time, clear work-life boundaries, and diversified sources of meaning and identity beyond work. The last point matters more than people realise. When work is your only source of purpose and identity, you’re vulnerable. Cultivating non-work relationships, hobbies, and activities creates resilience. If work becomes temporarily unbearable, you have other sources of meaning to draw from.
The Role of Family and Social Support in Burnout Recovery
Research consistently shows that perceived family support protects against both burnout development and cognitive decline during burnout. Social connection isn’t a nice-to-have — it’s essential infrastructure for recovery. Longitudinal studies show that family support moderates the relationship between burnout and cognitive performance. People with strong support maintain better cognitive function even when experiencing high work stress.
However, burnout often damages your capacity for social connection. You withdraw precisely when you need people most. Energy depletion makes social interaction feel impossibly demanding. Start small. One brief conversation with someone you trust. Ask for practical help rather than trying to manage everything alone. Accept that you’re temporarily operating with reduced capacity and need support systems you might normally provide to others. For more on the cognitive benefits of social connection, see my article on why your brain needs people.
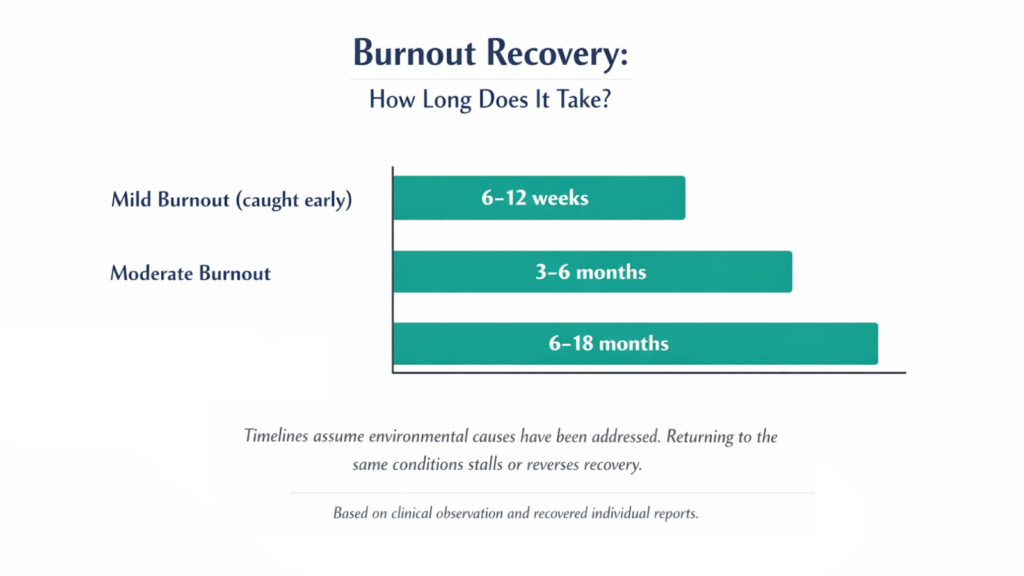
How Long Does It Take to Recover From Mental Burnout?
Everyone asks this. The answer is frustratingly variable: weeks to years, depending on severity and whether environmental factors change. Research suggests subjective cognitive fatigue can persist for three years after diagnosis, though this doesn’t mean continuous severe impairment — it means lingering vulnerability and slower recovery than acute stress.
Anecdotal reports from recovered individuals suggest: mild burnout (caught early) recovers in six to twelve weeks with proper intervention; moderate burnout typically needs three to six months; severe clinical burnout often requires six to eighteen months for substantial recovery, with lingering vulnerability for longer. These timelines assume you’ve actually addressed environmental causes. If you return to the same toxic conditions, recovery stalls or reverses.
Progress isn’t linear. You’ll have good days and terrible days. The trend should be upward over weeks and months, even if daily variation is substantial. Key recovery markers: improved sleep quality, ability to concentrate on complex tasks for longer periods, emotional regulation improves, physical energy returns, interest in previously enjoyable activities resurfaces, and you can handle normal setbacks without catastrophising.
QUICK WIN:
Track your energy level on a simple 1–10 scale each evening for two weeks. Don’t try to change anything yet — just observe. Most people find the data more nuanced than their memory suggested: certain days, times, or activities consistently correlate with higher or lower energy. This information is the starting point for making targeted changes.
Warning Signs: When to Seek Professional Help
Some situations require professional intervention beyond self-management. If you are experiencing thoughts of suicide or self-harm, please seek immediate help — contact your GP, call 111, or reach the Samaritans on 116 123 (free, 24/7). Burnout can overlap with clinical depression, and when it does, it requires medical treatment.
If cognitive impairment is severe enough to impair safety — difficulties driving, operating machinery, or making critical decisions — consult a healthcare professional immediately. If you’ve attempted recovery strategies for eight to twelve weeks without any improvement, professional assessment is warranted. You might have comorbid conditions requiring specific treatment.
Occupational health psychologists, clinical psychologists with workplace specialisation, and psychiatrists familiar with burnout can all provide appropriate assessment and treatment. General practitioners may prescribe antidepressants, which can help comorbid depression but don’t address burnout’s environmental causes.
Prevention: Building Long-Term Resilience Against Mental Burnout
Once recovered, preventing recurrence becomes priority. This requires ongoing vigilance about early warning signs and non-negotiable recovery practices.
Monitor your energy budget. Track subjective energy levels weekly. When you notice sustained decline over two to three weeks, investigate causes immediately. What’s changed? Workload increased? Sleep degraded? Social isolation increased? Recovery time decreased? Early intervention prevents crossing into clinical burnout. Mild depletion recovers quickly. Clinical burnout requires months.
Non-negotiable recovery time. Build regular recovery into your schedule as permanently as you build work commitments. Exercise, sleep, social connection, hobbies — these aren’t optional extras when you have time. They’re infrastructure that enables sustainable performance.
Coach yourself through difficult periods. Be proactive in improving things that are draining you. Try coaching yourself to discover healthier choices for yourself.
Diversify identity and meaning. Develop sources of purpose beyond work. Relationships, creative pursuits, community involvement, physical challenges. When work is difficult, these provide meaning and energy that sustain you.
Regular stress management practice. Don’t wait until you’re burnt out to implement stress management. Build practices now that will buffer you during difficult periods. For evidence-based techniques, see my guide on stress management for mental performance.
Conclusion: How to Recover From Mental Burnout Requires Real Change
Mental burnout isn’t a character flaw or personal failing. It’s a predictable response to a chronic mismatch between environmental demands and available resources. The cognitive impairments are real — measurable deficits in memory, attention, and executive function that affect your work and life. But these changes are reversible with proper recovery.
Recovery requires three elements: individual symptom treatment (rest, exercise, stress management, cognitive rehabilitation), environmental modification (changing the workplace factors causing burnout), and time (measured in months, not weeks). Most burnout interventions focus exclusively on individual coping whilst ignoring environmental causes. This is like treating smoke inhalation whilst leaving someone in a burning building. You need both symptom treatment and environmental change.
If you’re currently burnt out, the most important message is this: recovery is possible, but only if you take it seriously. You cannot think your way out of a state of cognitive impairment. You need a systematic restoration of depleted resources. Start with stabilisation — stop getting worse, then rehabilitation — rebuild capacity, then environmental modification — address root causes. This process takes months, not weeks. That’s not pessimism — it’s realistic expectation-setting that prevents demoralisation when recovery isn’t instant.
Your brain has a remarkable capacity for repair and adaptation. Given proper conditions — reduced demand, adequate resources, sufficient time — it will recover. Those decisions are easier when you understand what’s at stake. Burnout isn’t just being tired. It’s a measurable cognitive impairment that affects every aspect of your work, relationships, and life. Recovery isn’t self-indulgence. It’s neurological rehabilitation. Take it seriously. Your brain deserves proper care.
For additional strategies to optimise cognitive performance and prevent burnout, see my comprehensive guide on how to improve mental performance.
RESOURCES:
I only recommend resources that I either use personally or have researched and feel are genuinely helpful for my readers. Resources sometimes contain affiliate links; if you purchase through these, I may earn a small commission at no extra cost to you.
Recommended reading
The Upside of Stress — Kelly McGonigal. Reframes the relationship between stress and performance using the same research base that underpins this article — particularly useful for the prevention phase of burnout recovery. Paperback
Why Zebras Don’t Get Ulcers — Robert Sapolsky. The definitive accessible account of chronic stress biology — essential background reading for understanding what burnout is actually doing to your brain and body. Paperback
Related articles
Stress Management for Mental Performance — Evidence-based techniques that directly address the stress physiology underlying burnout.
Sleep and Cognitive Function — Why protecting sleep is foundational to burnout recovery and prevention.
Social Connection and Brain Health — How meaningful connection buffers against burnout and supports cognitive recovery.
Mindfulness for Focus — Practical mindfulness techniques for reducing the cognitive load that accelerates burnout.
How to Improve Mental Performance — The complete framework for cognitive optimisation once you’ve recovered.
I'm Simon Shaw, a Chartered Occupational Psychologist with over 20 years of experience in workplace psychology, learning and development, coaching, and teaching. I write about applying psychological research to everyday challenges - from habits and productivity to memory and mental performance. The articles on this blog draw from established research in psychology and behavioural science, taking a marginal gains approach to help you make small, evidence-based changes that compound over time, allowing you to make meaningful progress in the areas you care about most.





